
Pet Owner Information
Hip Luxation
What is Hip Luxation?
Hip luxation occurs when the femoral head or “ball” of the “ball-and-socket” joint comes out of the acetabulum or “socket”. In most cases, hip luxation is caused by major trauma, such as being hit by a car, kicked by a horse or cow, or falling from a height.
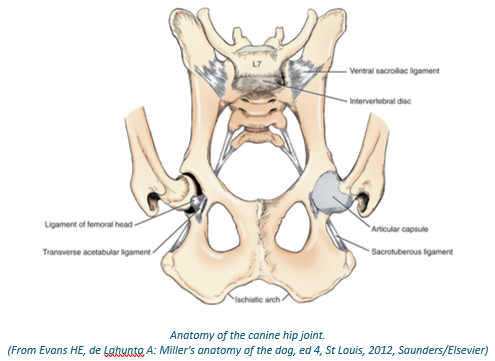
The normal hip joint is stabilised by primary and secondary stabilisers:
Primary stabilisers
- The ligament of the femoral head, which runs between the top of the femoral head and the base of the acetabulum (i.e. between the ball and the socket)
- The joint capsule that surrounds the joint
- The rim of the acetabulum
Secondary stabilisers
- Periarticular muscles (muscles surrounding the joint)
Traumatic hip luxation causes rupture of the ligament of the femoral head and tearing of the joint capsule in most cases, as well as tearing of muscular support in some cases.
Atraumatic hip luxation can also occur. Dogs with atraumatic hip luxation may be predisposed to hip luxation because of poor hip conformation (i.e. shallow hip joints in dogs with hip dysplasia or a deficient transverse acetabular ligament), although the exact mechanism is not confirmed in many cases.
Diagnosis of Hip Luxation
Hip luxation is diagnosed based on lameness, a characteristic limb position, hip pain, distorted anatomy (i.e. palpation of the femur in a craniodorsal position relative to normal) and radiographs. Radiographs confirm the presence and direction of hip luxation and allow for surgical planning.
Most cases of hip luxation have sustained major trauma, and radiographs may also be used as a screening tool for other traumatic injuries (chest, abdomen and other limbs). A CT scan will be recommended in some trauma cases as this is a more sensitive way to assess multiple body systems and to screen for small fractures to the hip joint, which can occur at the time of luxation and have a major impact on potential repair options.
Treatment of Hip Luxation
Non-surgical management of hip luxation may be considered in select cases of both traumatic and atraumatic luxation. This involves so-called closed reduction of the luxated hip under anaesthesia to replace the femoral head back into the acetabulum. In specific cases of atraumatic hip luxation, this may be followed by application of a bandage known as hobbles to prevent the back legs from splaying.
The outcome of closed reduction is variable with success in up to 50% of cases. If the hip re-luxates or if there are other injuries, surgical management is indicated.
There are three main surgical options for the management of hip luxation:
- Toggle rod stabilisation – this involves placing an anchor into the base of the acetabulum and using a braided suture to re-create the ligament of the femoral head that is passed through a bone tunnel in the femur. This is the treatment of choice for most traumatic hip luxations and some atraumatic hip luxations and is successful in 85-90% of cases.
- Total hip replacement (THR) – this is a salvage surgery to replace an irreversibly damaged hip joint. This may be recommended in chronic cases, or those with concurrent fractures to the femoral head. If THR is required, referral to specific facilities providing this surgery would be recommended
- Femoral head and neck excision – this is a salvage surgery where the femoral head is removed. This removes bony contact between irreversibly damaged surfaces and allows formation of a pseudo- (“false”) joint. This procedure can facilitate pain-free function; however, a persistent mechanical lameness will often result.

Postoperative Care
Toggle-rod stabilisation requires 6-8 weeks of strict crate or room confinement while the damaged joint capsule and periarticular muscles repair. Radiographs will be performed after the recovery period to ensure the implants remain in place.
Femoral head and neck excision requires 2 weeks of strict confinement following surgery, followed by a graduated exercise program. This procedure relies on muscular support of the limb, so maintaining muscle mass is an essential part of postoperative management.
Outcome
The outcome following toggle-rod stabilisation is excellent in most cases. Animals will develop a degree of osteoarthritis following any traumatic injury to a joint including hip luxation and, as such, life-long strategies to manage this will be important (weight control, exercise moderation, medical management).
Complications are uncommon following toggle-rod stabilisation; however, complications to be aware of are re-luxation (10-15%), infection (<5%) and implant irritation of soft tissues (rare).
The outcome following femoral head and neck excision is more variable; however, in most cases a functional and pain-free outcome can be achieved although a symmetrical gait should not be expected.